
TCA, vol 14. Do masks work? part 2.
Math models of masking.


Whether or not wearing facemasks prevent COVID-19 tranmission in a population has been a hot debate. When debates happen, I always go back to the science for direction. Unfortunately, the science in this case has not offered much clarity. There are multiple studies, using many different designs, to determine masking efficiency and they have had varying results.
Part of the problem comes from how differently these studies are designed. In volume 13, I describe a “difference in differences” study looking at masking in public schools. This type of study is observational: a researcher watches things happen in a real-world scenario and tries to make heads or tails of it. As you can imagine, real life scenarios are full of variables. Not the least of which is how unpredictable human behavior can be.
Another way to “test” mask efficiency is through mathematical modeling. In this type of study, a researcher uses probability and statistics to predict what might happen. Take this study in Science: Face masks effectively limit the probability of SARS-CoV-2 transmission. Here, researchers assume that surgical masks will filter out 30-70% of inhaled particles. Next, they create a hypothetical situation where a person is in a “virus-rich regime” or a “virus-limited regime”. A virus-rich regime would be like an indoor situation where there are sick people, like a hospital. A virus-limited regime would be more like outdoors, or a very well ventilated indoor area. Then, they use MATH to figure out whether or not masking would protect you from infection. The equation in this case is:

Pinf is the probability of infection, Psingle is the infection probability of a single virus, and Nv is the number of viruses you inhale. Then, they scaled the model below to include “infectious dose 50” which is basically the number of viruses you need to be exposed to in order to get an infection. The ID50 has not been conclusively determined for COVID-19, but I’ve seen published ranges as low as 500, 700, and up to several thousand viruses. This means that you would have to inhale between 500 and several thousand COVID-19 viruses in order to get sick.
Here is what their model found:

On the left, the black line represents the probability you will get infected: as the line decreases, you are less likely to get infected. The two dots on the line represent the number of viruses you inhale without a mask (Nv) and the number of viruses you inhale while wearing a mask (Nv, mask) which would be reduced by 30-70%. As you can see from the data in panels A and B, when a person is in a “virus-rich regime” wearing a mask will reduce the number of viruses you are exposed to, but the reduced number is still ABOVE the ID50… which means you’ll still get infected even though you are wearing a mask. The mask is working, but the number of viruses in the room is so high, that even a 30-70% reduction is not enough to protect you.
In panels C and D, we see what happens when a person is in a “virus-limited regime” like outdoors or in a well ventilated indoor space. Mask wearing reduces the number of viruses you inhale by 30-70% and now that number is actually SMALLER than the ID50, meaning you wont get infected if you are wearing a mask. The mask reduces the number of viruses you inhale from “enough to make you sick” to “not enough to make you sick” because the number of viruses in the room was not that high to start with.
This is very interesting to me since it might explain why some observational studies show benefits of mask wearing, and others do not. If one study was in a “virus-rich regime” and another study was in a “virus-limited regime” then this model explains why masks would work in the second, but not the first, scenario. And, the researchers of this study indicate that mask wearing could become much more effective if you turn a “virus-rich" regime into a “virus-limited” one by either social distancing or improving ventilation.
Next they tried to insert some specific COVID-19 parameters and look at what would happen if you compared universal masking, masking only the infected people (source) or masking only uninfected people (wearer).
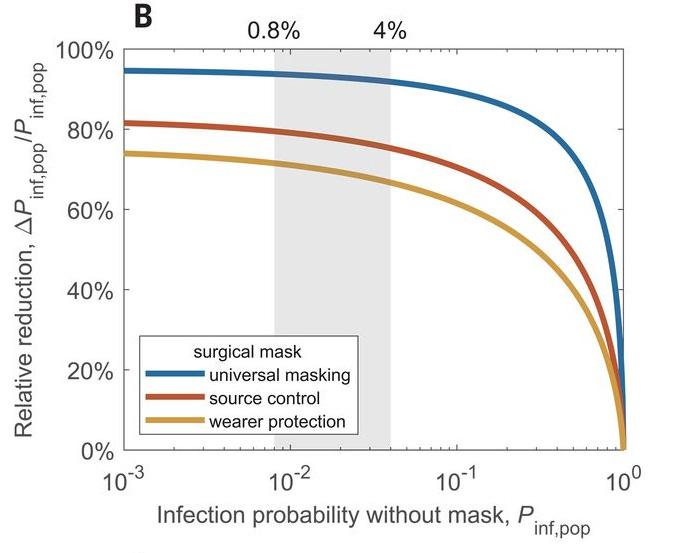
The gray shaded zone indicates the range of probability that someone will contract COVID-19, all things being equal. The blue line indicates the reduction in infection when everyone is masked, the red line indicates the reduction when only the sick are masked, and the yellow line indicates the reduction when only the well are masked. So, their models predict universal masking will give you upwards of 90%+ protection from infection; source masking only will provide ~80% reduction of infection; and wearer masking will provide ~70% reduction in infection. (Note: this assumes the basic probability of getting COVID is 0.8% to 4%: the shaded gray area. That’s a pretty big assumption. If you follow the color lines out to the right, you can see that masks offer much less protection if the odds of you getting infected maskless is higher).
This all sounds promising, but kind of falls apart when you compare it to real-world data, which has never shown masks to be this effective. Remember, these are all theoretical modeling systems that take almost nothing into account like: incorrect fit of mask, incorrect usage of mask, type of mask, strain of virus, people’s behavior, etc, etc, etc. So, I guess this is a kind of “all things being perfect” theoretical prediction of what masks could do if they were always perfectly used.
And that, my readers, is the downfall of modeling studies. Its not real.