

TCA, vol. 37: Rising cancer rates in the young.
TCA, vol. 37: Rising cancer rates in the young.
It's not just for royals.

Recent alarming headlines about an increase in “early onset” cancer have dominated the news since the American Cancer Society released their 2024 cancer statistics in January. While more people are surviving a cancer diagnosis, and the rates of cancer in “older” people is not increasing, an increase was indeed seen in “young” people’s diagnosis of breast, colorectal and lung cancers.
Another surprise from this study was that the definition of “young” when it comes to cancer is ages 18-50. I’m officially young!
Cancer is not just one disease.
The phrase “a cure for cancer” has always annoyed me because it implies that all cancers are the same and that there will be one treatment or drug that cures everyone. All cancers are different. All people are different. All people’s cancers are different.
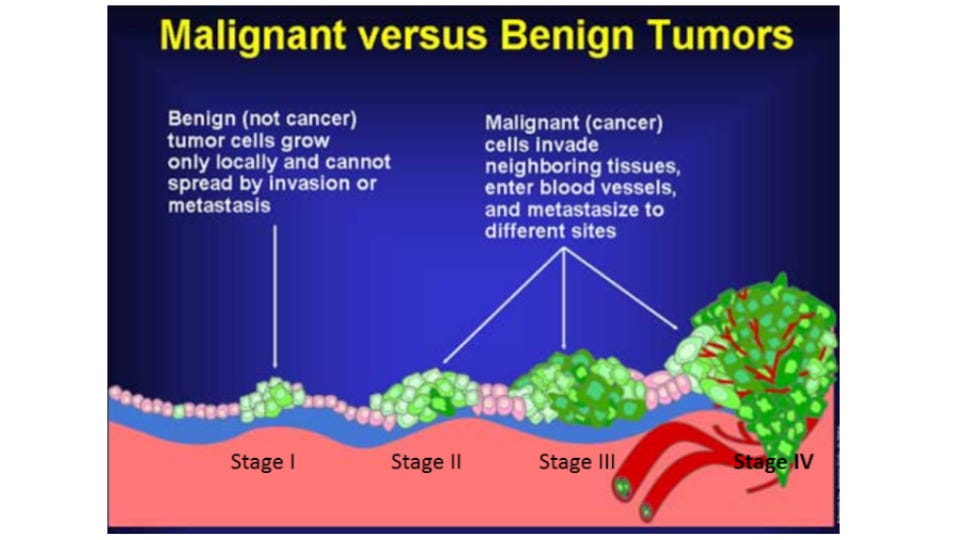
Cancer refers to a situation where your body’s cells go rogue and start dividing uncontrollably, and invade into other tissues. This is different from a benign (not dangerous) growth where cells also divide inappropriately but do not invade or cause damage. Examples of these are common, like skin tags, moles and fibroids.
There are dozens, if not hundreds of reasons why a cell might start to divide too often, creating a lump of identical and abnormal cells. Most of them, however, have something to do with the cell cycle.
Flashbacks to high school biology!

The cell cycle is a series of steps where one cell grows, duplicates its DNA and divides into two cells. It’s controlled very tightly in the body. There are times when the cell cycle might need to be fast because you need more cells quickly: creating more immune system cells in response to an infection; wound healing; development of the fetus. But most of the time the cell cycle is slow and predictable, simply replacing old and dying cells with new fresh ones.
The cell cycle is controlled in two general ways: oncogenes that speed up the cell cycle (stepping on the gas) and anti-oncogenes (also called tumor suppressor genes) that slow down or stop the cell cycle (stepping on the brakes). There are many genes that fall into either one of these categories. If a situation occurs where oncogenes are working too hard, its like stepping hard on the gas… accelerating the cell cycle and possibly causing a tumor. Alternatively, situations occur where the anti-oncogenes are not working well enough, like releasing pressure on the brakes and again, a tumor could form.
What are these situations? Most often it is a mutation in one of these genes either increasing it’s action (oncogene) or decreasing its action (anti-oncogene). Mutations can happen because of infections with certain viruses like HPV, exposure to carcinogens like cigarettes or UV light, or they are pre-existing genetic mutations and passed down in the family line.
Let’s say your DNA has a mutation in it… does that mean cancer is inevitable? No. Because it takes more than just a mutation to cause cancer. The mutation causes the cell to divide too fast, but there are other “mistakes” that need to happen to result in a cancerous tumor to form. The cell needs to keep on dividing (just a few quick trips through the cell cycle wont do it); the tumor needs to avoid detection by the immune system which kills tumor cells in addition to bacteria and viruses; the tumor needs to grow blood vessels to feed all these new cells with oxygen and sugar; and the tumor needs to have enzymes or proteins that allow it to damage, invade other areas or spread around the body (metastasis). All of these things have to happen in order to go from a benign growth to a metastatic malignant tumor.
So let’s do the math. There are over 100 oncogenes known, and over 1000 anti-oncogenes. A given tumor can have mutations in any one of these genes, and often multiple mutations in different genes in unique combinations. If you took a tumor out of one woman’s breast and compared it to the tumor of another woman, likely those two breast cancers would be very different in which genes were mutated and in which combinations.
While there are trends, no two tumors are alike. It’s personal.
Let’s look at the big picture.
I’d like to show you the actual data from the ACS January report so you can have some context. All of the following figures are taken from the American Cancer Society Facts and Figures 2024.

The estimated total number of expected cancer diagnoses in America for 2024 is 2 million, up from 1.9 million last year. For males, prostate, lung, colorectal and urinary are the top five. For females, breast, lung, colorectal and uterine are the top five.
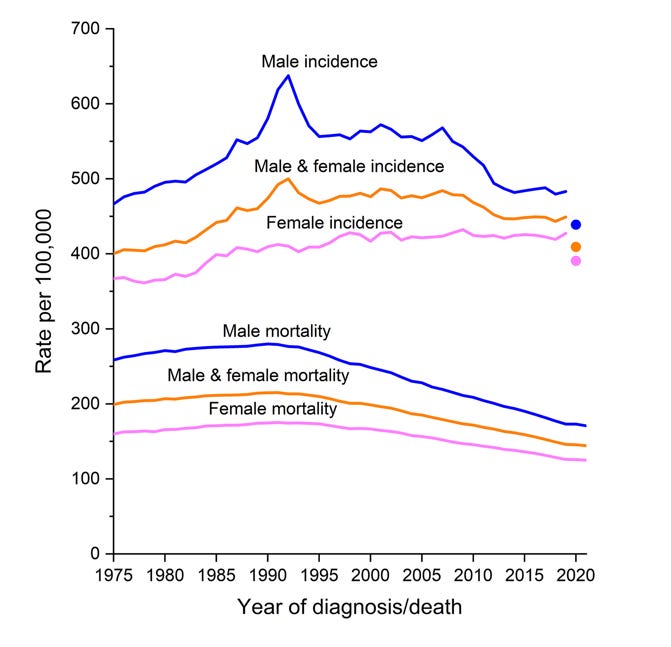
The graph above needs a bit of explaining. The top three lines show the incidence in new cancer diagnoses in males (blue), everyone (yellow), and females (pink) from 1975-2020.
Looking at the lines, male incidence is slightly up recently, although down significantly from years prior (the huge spike in 1990 was from new prostate cancer screening techniques detecting cancer better, not from an actual increase in cancer incidence). Female cancer incidence has crept up slowly across all the years.
See the three dots on the far right side, correllating to 2020? Those are the numbers from 2020, they just didn’t connect the lines to the new numbers. If you did, it would look like all three lines went down a lot between 2019 and 2020. However, they believe that the 2020 numbers are artificially low because of the pandemic preventing routine cancer screenings and new diagnoses. They expect that to be a blip, and rates to be up after the pandemic ended.
The good news comes from the bottom part of the graph. Dying from cancer is down in all age groups due to better screening, a reduction in cigarette smoking and new treatments.
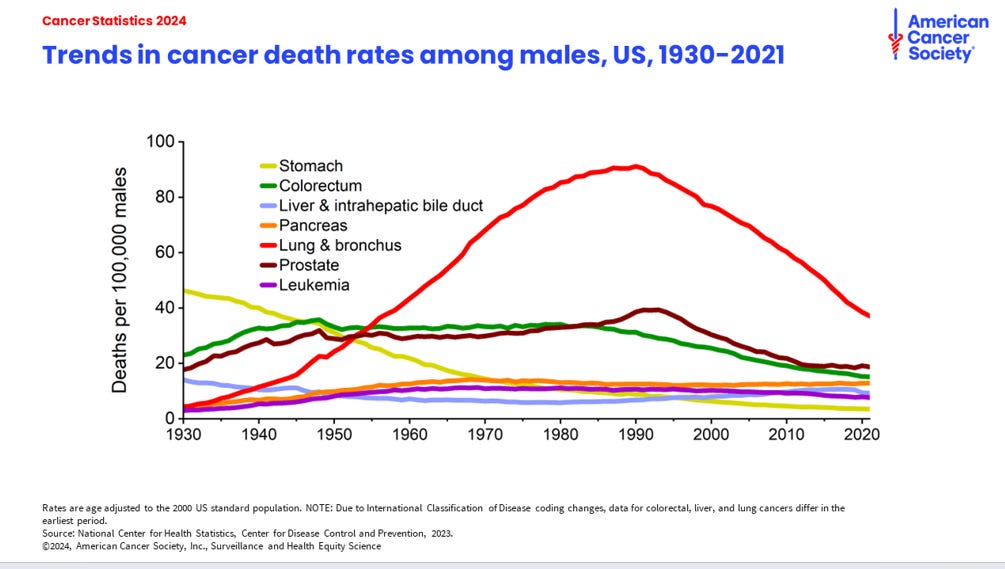
And this reduction in mortality is across all different types of cancer. In men:
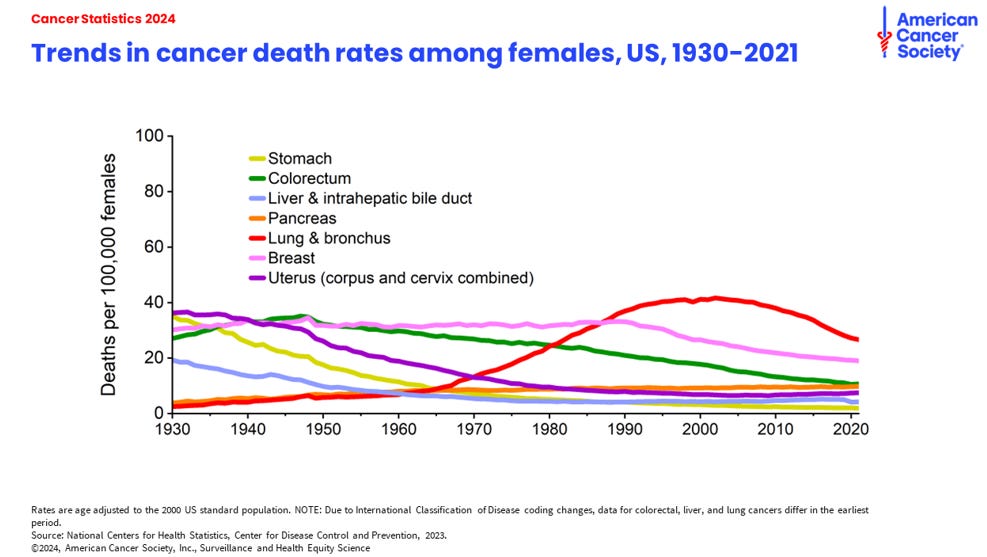
And in women:
This good news is not for everyone though. The mortality rate from cancer is not equal across all demographics. Although men are more likely to die than women in every group, American Indian/Alaska Natives and Black Americans carry a disproportional burden of cancer mortality.
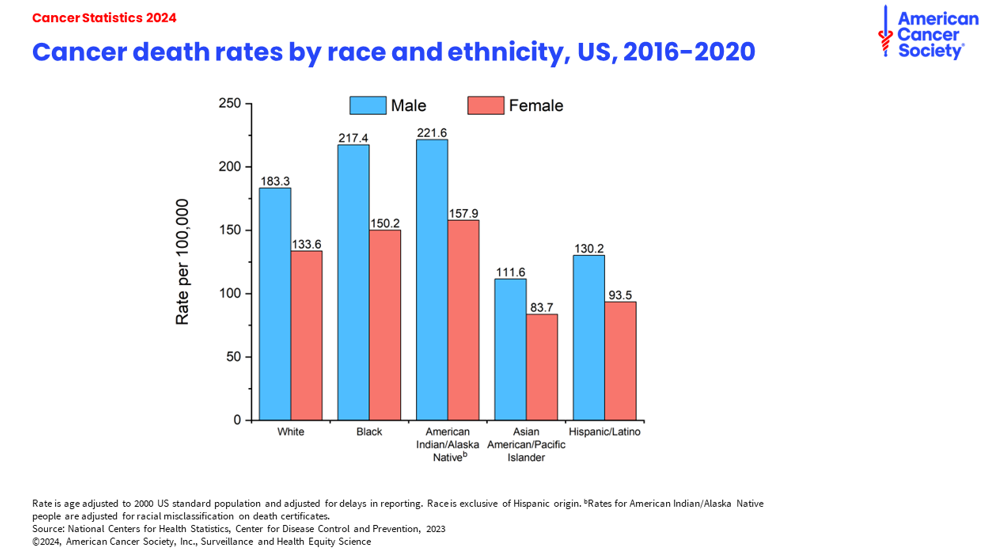
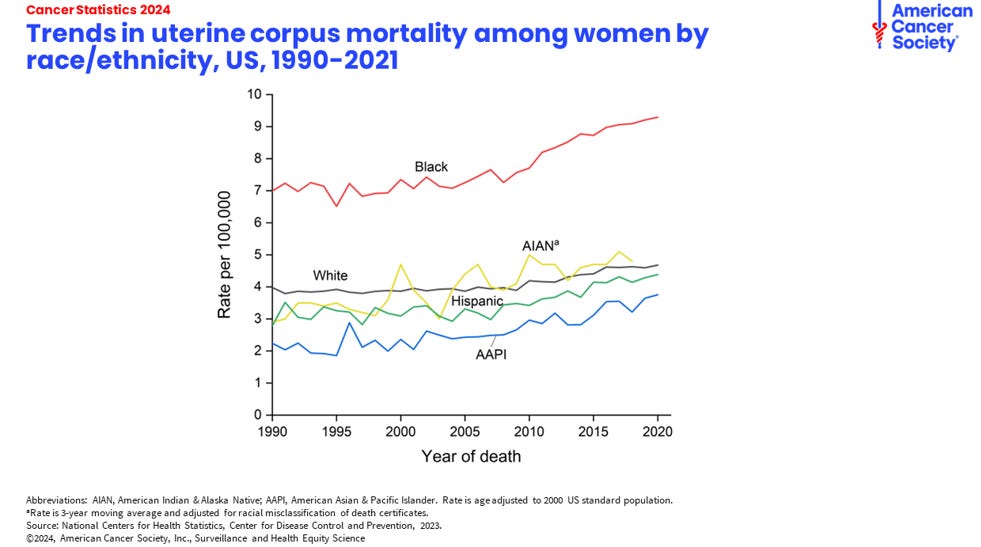
Black women, especially. Their rate of dying from uterine cancer is 2x that in white women.
And black women are 41% more likely to die of breast cancer than white women, even though they are less likely to even get breast cancer in the first place. This disparity is thought to come from inequalities in wealth and access to cancer prevention, screening and treatment. Also, black women are less likely to get a mammography referral from their provider than whites, less likely to get a follow up after an abnormal screening, and less likely to get aggressive treatment or be included in new treatment trials.
Dang.
Ok, back to the increase in “early onset cancer”.
Although age is still the number one determinant in whether or not you’ll get cancer, rates of cancer are not trending equally in all age groups. They broke it down into three age groups (no figure sadly) for diagnoses between 2019-2020.
65 and older adults (the largest group of cancer diagnoses) saw an overall decrease. 61% of new cancer diagnoses in 2019 were 65+, but decreased to 58% in 2020, even though the number of people in this age group actually increased in the overall population from 13-17%.
50-64 year olds. Cancer diagnoses went up from 25% to 30% , but there are also just more people in this age group in America. 50-64 year olds now make up 19% of the population, up from 13%. The number of cancer diagnoses increased commensurate with the overall number of people in this age group, meaning no rise in cancer incidence overall.
18-50 year olds. The only group that saw an increase in the rate of cancer diagnoses despite any changes in overall population size.
The early onset cancers of concern are breast, colorectal (and other cancers of the digestive system like stomach or pancreas) and lung. There doesn’t seem to be one answer that explains it all, but rather a combination of reasons.
Younger people are less likely to get screened. Cancers go undetected and when they are eventually discovered, are already in an advanced state.
Digestive cancers may be on the increase because of increasing obesity rates and a change in diet to a more processed and fatty diet with fewer fruits, vegetables and whole grains. Ozempic may be a game changer here, we’ll have to wait and see.
Increase in alcohol consumption across time in this age group.
However, there are other, more subtle, reasons that will take longer to figure out. There may be changes in the gut microbiome that contribute to colorectal cancer. Studies are underway now looking at tumors from early-onset cancers and those from 65+ year olds to determine if there is something genetically different.
HPV has its own story.
Human Papilloma Virus is the most common sexually transmitted infection in the world, and almost all sexually active people will contract it at some point in their lives. Most of the time it causes no disease at all. Sometimes it causes warts. In a small percentage of cases it causes anal, penile, vulvar, cervical or oro-pharyngeal (back of throat) cancers. Even though the percentage of HPV infections that cause cancer is low, the actual numbers of HPV-caused cancers are high because so many damn people are infected. HPV is now the leading cause of throat cancer, surpassing smoking.
But there is some good news.
The rate of cervical cancer in women age 20-24 years has decreased 65% largely due to Gardasil, the HPV-vaccine. The rate of cervical cancer has dropped a little more modestly for 25-29 year olds, about a 6.4% decrease every year. Unfortunately, cervical cancer rates among 30-44 year olds has actually gone up 1.7% per year. These numbers correlate strongly with the rate of Gardasil vaccination in each age group. The older you are, the less likely you are to have been vaccinated.
Because of widespread usage of Gardasil, Australia and the UK are on track to completely eliminate cervical cancer by 2035 and 2040, respectively. The vaccination rates are lower in the USA, so it will take us longer, but it is possible.
Stay happy, healthy and informed,
Jessica at TCA
American Cancer Society. Cancer Facts and Figures, 2024.
Siegal, R. et al. Cancer Statistics, 2024. CA: A Cancer Journal For Clinicans. Jan 2024.
Katella, K. What to Know About Rising Rates of 'Early-Onset' Cancer. Yale Medicine. Mar 2024
Ledford, H. Why are so many young people getting cancer? What the data say. Nature. Mar 2024.
NHS sets ambition to eliminate cervical cancer by 2040. NHS England.